High-frequency Ultrasound Imaging for Cardiac Fibers
3D Ultrasound and MR Diffusion Tensor Imaging
Simulated Ultrasound Image from MR Diffusion Tensor Image
Cardiac Fibers in Pig Hearts
Heart Failure
Heart failure affects ≥5 million people in the USA. About half the people who develop heart failure die within 5 years of diagnosis. It is a leading cause of hospitalization, death, and disability in developed countries, creating a significant social and economic burden for patients and health care systems. The treatment costs are estimated to be $32 billion each year. While the underlying cause of heart failure may be quite varied, common features of the failing heart include myocyte hypertrophy and fibrosis. Currently, most methods for the detection of heart failure focus on geometric abnormalities utilizing MRI, ultrasound and CT. Although there have been tremendous improvements in diagnostics for cardiac disease, many of the current techniques are useful only when significant cardiac dysfunction is present. It is well documented that early detection can rescue patients from acute failure and save lives. Early detection of ventricular dysfunction, before progression to full heart failure, is essential to improve patient outcomes.
Cardiac Fibers
Cardiac fibers directly affect the mechanical and physiological properties of the heart. During the cardiac cycle from systole to diastole, cardiac fibers are the basic units that pump blood from the ventricles into circulation. Cardiac fiber orientation plays an important role in determining the stress distribution within the myocardial walls. Abnormal cardiac fiber orientations in heart failure patients adversely impact cardiac function and also contribute to arrhythmias that can lead to sudden death. Mapping cardiac fiber orientation enables monitoring of the development and progression of heart failure and provides insight into the mechanism of heart failure for early detection. It is reported that cardiac fiber angles changes through the wall from epicardium to endocardium and that the angles increase from systole to diastole. In a normal heart, the change of fiber orientation is from around -75° at the epicardium to +75° at the endocardium.
Alterations of
cardiac fiber orientation can have significant pathological consequences. Animal studies have shown that
ventricular transmural fiber rotation was significantly changed in hypertrophic versus normal hearts and that
muscle fiber stress and strain across the ventricular wall are very sensitive to the transmural distribution of
helix angle. During heart beating, the fiber angles in systole are increased through the wall relative to their
counterpart in diastole.
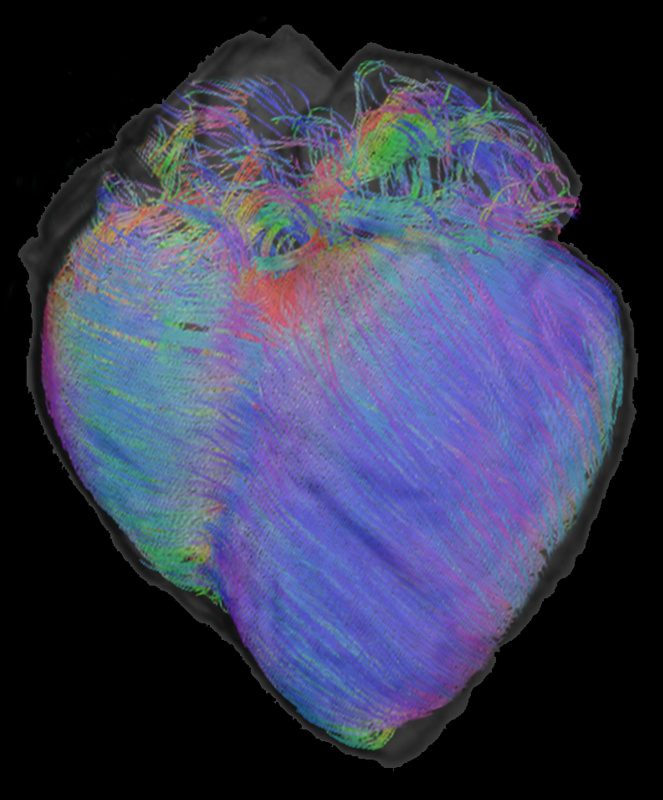
Fiber reconstruction superimposed with T1 MRI.